This week is dedicated to composing a results section that conveys, ultimately, the end goal of our year-long research project. Last week, I was able to finish the bulk of my data analysis. I spent this past week finding other trends within my data that could bolster my main conclusion or provide insight that is missing or lacking in this sphere of research. I found that on average, females improved more than males, teenagers improved more than young children, but younger adults improved more than older adults. Now, I am trying to outline a way to present these results to not overwhelm the readers, but rather keep them interested and informed.
I reviewed three studies that were about ADHD, two about neurofeedback therapy, that employed the same method of the t-test as mine. While I did a one-tailed, paired t-test, these studies used a one-tailed t-test, but the results are comparable to my study.
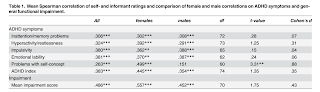
The first study, "Attention-Deficit/Hyperactivity Disorder (ADHD) in Adulthood: Concordance and Differences between Self- and Informant Perspectives on Symptoms and Functional Impairment" by Morstedt, Corbisiero, Bitto, and Stieglitz, investigated the differences in diagnostic measures to detect ADHD. The study presented the results in a table comparing the female and male correlations on ADHD symptoms. The t-value, degrees of freedom, and the p-value were recorded. Underneath, the results were not only summarized but explained in relation to each other. For example, it was identified under the table that males were more likely to rate the hyperactivity/restlessness symptom higher than females and other trends that can be siphoned from the raw data in the table. The t-values are described in comparison with each other, rather than stated independently with no context. I can use this when I convey my results, providing further explanation under a raw table. It is vital to have the t-values there, but, without an explanation, the significance would be lost on the readers. This study also broke down the results into different categories (first explaining the internal consistency measures, then the r-value, then the t-value). My research also has several parts that can be separated in a similar fashion (determining normal distribution, average score decrease, t-scores, and other trends).
The second study, "Efficacy of Neurofeedback treatment in ADHD: The effects on Inattention, Impulsivity, and Hyperactivity: A meta-analysis" by Arns, Ridder, Strehl, Breteler, and Coenen, aimed to find the effect of neurofeedback therapy on treating ADHD in comparison to stimulant medication. Something I could replicate in my own research is the way that this study presents the general results/main conclusion first, and then goes into results of the subcategories and other data found. Like my study, they noted the number of sessions, neurofeedback therapy site on brain, age of the participant, and what brain waves frequencies were targeted. After a table of this information, the results were depicted in paragraph style above a graph describing the results. I can similarly start with my greater conclusion about the comparison of reduction of ADHD scores between children and adults and reflect the results through a graph. Then I could go into the smaller conclusions or calculations (the specific scored categories that make up the ADHD scores and the other trends). I need to be able to tie the smaller conclusions back to the adult/child group comparison at the end.

 The third study, "The Effect of Neurofeedback Therapy on Reducing Symptoms Associated with Attention Deficit Hyperactivity Disorder: A Case Series Study" by Deilami, Jahandidedh, et al., aimed to measure the effect of 30 sessions of neurofeedback therapy on children 5-12 years old. Using graphs to depict the calculations with standard deviation and means of the results, the study went from the general conclusion to calculations and explanation. The results section of this paper was relatively short, describing the main conclusion with the dependent t-test in two quick paragraphs. I think a major problem with my results outline right now, as Mrs. Haag noted, is I have a lot of raw data and not enough consolidation of the information and connection back to the hypothesis and purpose of the paper. Using this study as reference, I can aim to make sure my results are not lost in calculations and are presented in a way that shows how they were found but also what they mean in easily understood terms.
The third study, "The Effect of Neurofeedback Therapy on Reducing Symptoms Associated with Attention Deficit Hyperactivity Disorder: A Case Series Study" by Deilami, Jahandidedh, et al., aimed to measure the effect of 30 sessions of neurofeedback therapy on children 5-12 years old. Using graphs to depict the calculations with standard deviation and means of the results, the study went from the general conclusion to calculations and explanation. The results section of this paper was relatively short, describing the main conclusion with the dependent t-test in two quick paragraphs. I think a major problem with my results outline right now, as Mrs. Haag noted, is I have a lot of raw data and not enough consolidation of the information and connection back to the hypothesis and purpose of the paper. Using this study as reference, I can aim to make sure my results are not lost in calculations and are presented in a way that shows how they were found but also what they mean in easily understood terms.
All these studies had in common the presenting of the raw data in a table, a table for calculations, and then a simpler, short explanation for the general conclusions. The studies started with a general conclusion, went into specifics of its discovery, and then tied it back to the general purpose. Graphs and tables were primarily used to show the relationships between the average differences and the t values. These are all elements I can incorporate into my results section to hopefully reflect the significance of my work in a clear way.
(810)
I reviewed three studies that were about ADHD, two about neurofeedback therapy, that employed the same method of the t-test as mine. While I did a one-tailed, paired t-test, these studies used a one-tailed t-test, but the results are comparable to my study.
The second study, "Efficacy of Neurofeedback treatment in ADHD: The effects on Inattention, Impulsivity, and Hyperactivity: A meta-analysis" by Arns, Ridder, Strehl, Breteler, and Coenen, aimed to find the effect of neurofeedback therapy on treating ADHD in comparison to stimulant medication. Something I could replicate in my own research is the way that this study presents the general results/main conclusion first, and then goes into results of the subcategories and other data found. Like my study, they noted the number of sessions, neurofeedback therapy site on brain, age of the participant, and what brain waves frequencies were targeted. After a table of this information, the results were depicted in paragraph style above a graph describing the results. I can similarly start with my greater conclusion about the comparison of reduction of ADHD scores between children and adults and reflect the results through a graph. Then I could go into the smaller conclusions or calculations (the specific scored categories that make up the ADHD scores and the other trends). I need to be able to tie the smaller conclusions back to the adult/child group comparison at the end.

 The third study, "The Effect of Neurofeedback Therapy on Reducing Symptoms Associated with Attention Deficit Hyperactivity Disorder: A Case Series Study" by Deilami, Jahandidedh, et al., aimed to measure the effect of 30 sessions of neurofeedback therapy on children 5-12 years old. Using graphs to depict the calculations with standard deviation and means of the results, the study went from the general conclusion to calculations and explanation. The results section of this paper was relatively short, describing the main conclusion with the dependent t-test in two quick paragraphs. I think a major problem with my results outline right now, as Mrs. Haag noted, is I have a lot of raw data and not enough consolidation of the information and connection back to the hypothesis and purpose of the paper. Using this study as reference, I can aim to make sure my results are not lost in calculations and are presented in a way that shows how they were found but also what they mean in easily understood terms.
The third study, "The Effect of Neurofeedback Therapy on Reducing Symptoms Associated with Attention Deficit Hyperactivity Disorder: A Case Series Study" by Deilami, Jahandidedh, et al., aimed to measure the effect of 30 sessions of neurofeedback therapy on children 5-12 years old. Using graphs to depict the calculations with standard deviation and means of the results, the study went from the general conclusion to calculations and explanation. The results section of this paper was relatively short, describing the main conclusion with the dependent t-test in two quick paragraphs. I think a major problem with my results outline right now, as Mrs. Haag noted, is I have a lot of raw data and not enough consolidation of the information and connection back to the hypothesis and purpose of the paper. Using this study as reference, I can aim to make sure my results are not lost in calculations and are presented in a way that shows how they were found but also what they mean in easily understood terms.(810)
